Oral Presentation ESA-SRB-ANZOS 2025 in conjunction with ENSA
Diagnostic Utility and Cost Analysis of Pragmatic Sequential Transcription Factor Immunohistochemistry in Adenohypophyseal-Immunonegative Pituitary Adenomas (128467)
Background: Since 2022, transcription factor (TF) immunohistochemistry (IHC) has been recommended for pituitary adenoma subtype identification.1 However, the routine use of TF IHC in clinical practice is variable due to financial and laboratory resource limitations.2 Our pilot study demonstrated that gonadotroph adenoma was the most prevalent revised diagnosis after retrospective additional TF IHC in adenohypophyseal-immunonegative pituitary adenomas.3 We aimed to conduct a validation study, perform a cost analysis of our proposed pragmatic sequential TF IHC approach, and quantify the routine use of TF IHC in clinical practice.
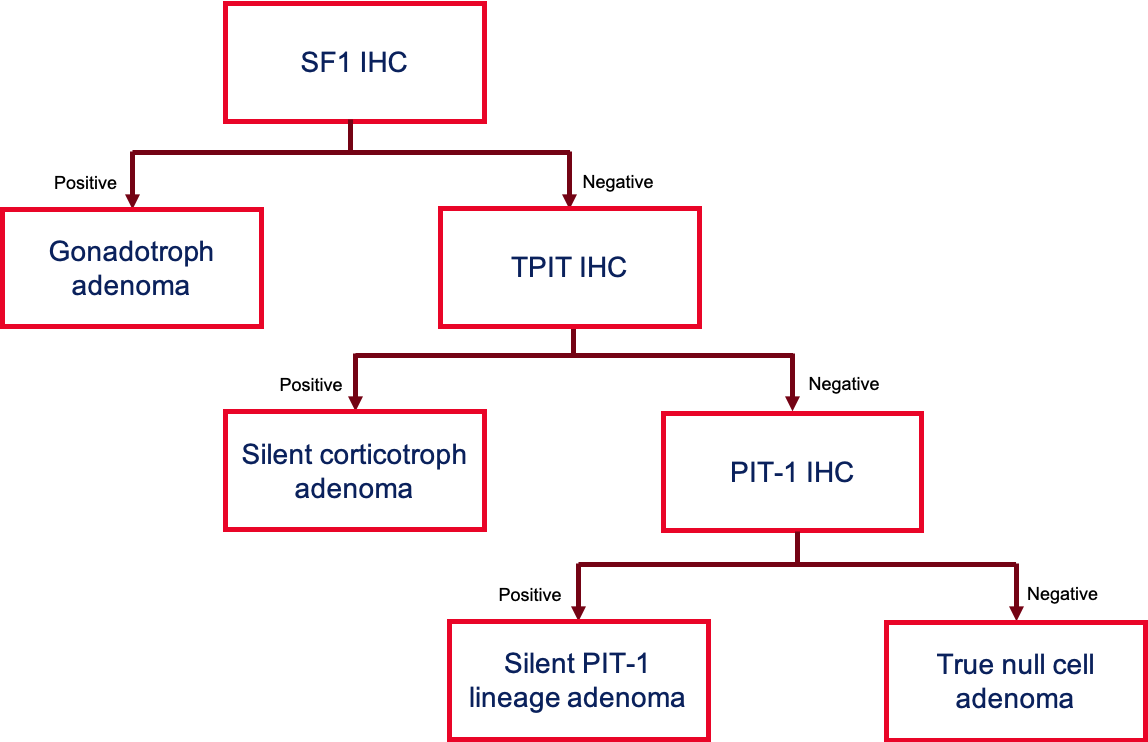
Methods: In the most recent 100 patients diagnosed with null cell adenomas without prior TF IHC at our tertiary pituitary hospital, SF1, TPIT, and PIT-1 were performed. The diagnostic accuracy of our pragmatic sequential TF IHC approach (SF1, followed by TPIT, then PIT-1) was simulated (Figure 1), with a cost analysis comparing it to traditional TF IHC. A telephone survey of hospitals performing pituitary surgery across Australia and New Zealand was conducted to assess the routine TF IHC use.
Results: Ninety-six patients labelled as null cell adenomas were available for retrospective additional TF IHC. The most commonly revised diagnosis was gonadotroph adenomas (56.3%), followed by corticotroph adenomas (15.6%), plurihormonal adenomas (11.5%), and PIT-1-lineage adenomas (1.0%). The pragmatic sequential TF IHC approach yielded 88.5% diagnostic accuracy, with a cost reduction of $6,150 (48%) compared to the traditional TF IHC approach. The telephone survey revealed that 42.9% (n=9/21) of hospitals do not perform routine TF IHC.
Conclusion: We validated our finding that the majority of the adenohypophyseal-immunonegative pituitary adenomas are gonadotroph adenomas. Three years post-diagnostic paradigm shift, over 40% of hospitals do not routinely perform TF IHC. In resource-limited settings, our pragmatic TF IHC approach may accurately subtype adenohypophyseal-immunonegative pituitary adenomas in approximately 90% of cases at nearly half the cost of traditional methods.
- Asa SL, Ezzat S. Pituitary carcinoma: reclassification and implications in the NET schema. Endocr Oncol. 2022;2(1):R14-r23.
- Lenders NF, Earls PE, Inder WJ, McCormack AI. The evolution in pituitary tumour classification: a clinical perspective. Endocrine Oncology. 2023;3(1):e220079.
- Park YA, Christie M, King J, Shen A, Yates C. Prevalence of non-functioning pituitary adenoma subtypes at a Melbourne quaternary centre and underdiagnosis of gonadotroph adenomas [Conference presentation]. Australia and New Zealand Pituitary Alliance; Gold Coast, Queensland, Australia. 2024.