Poster Presentation ESA-SRB-ANZOS 2025 in conjunction with ENSA
When imaging fails, the vein prevails: Investigating postmenopausal hyperandrogenism with adrenal and ovarian vein sampling (#169)
Aims
To evaluate the role of selective adrenal and ovarian vein sampling in postmenopausal women with significant hyperandrogenism where conventional imaging fails to localise the source of androgen excess.
Methods
We present two postmenopausal women with virilising symptoms and markedly elevated serum testosterone levels. Both underwent comprehensive biochemical assessment and cross-sectional imaging, which failed to identify a clear source. Adrenal and ovarian vein sampling (AVS/OVS) was subsequently performed to localise androgen production and guide management.
Results
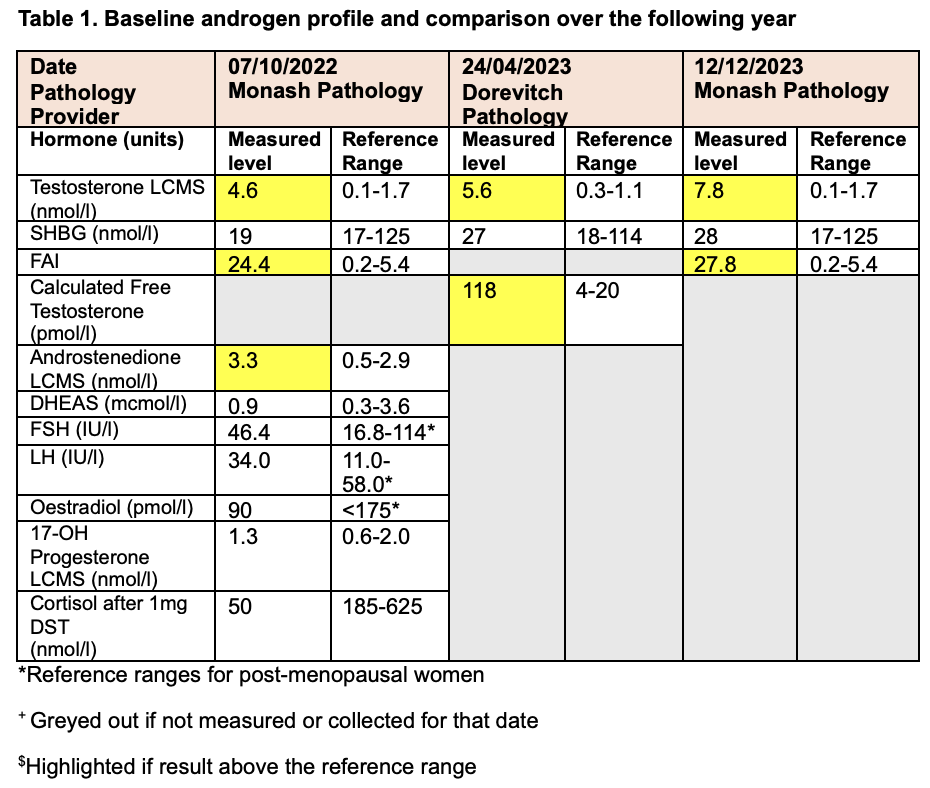
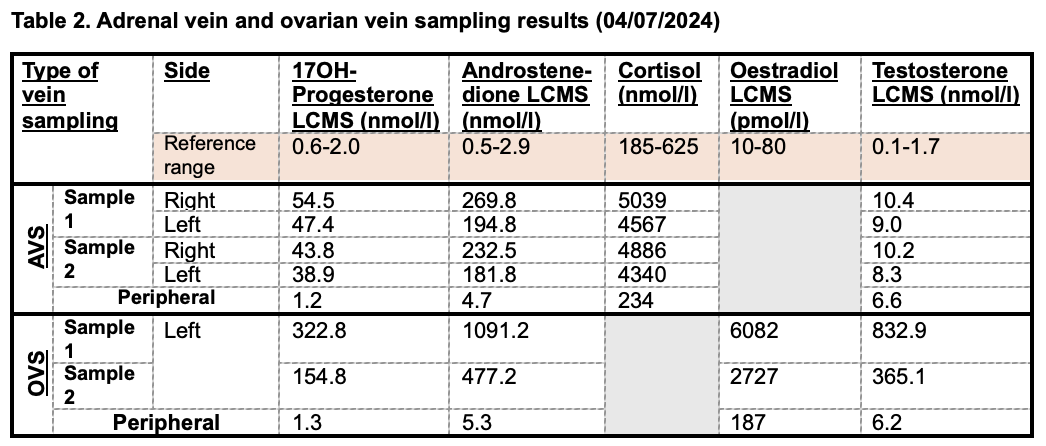
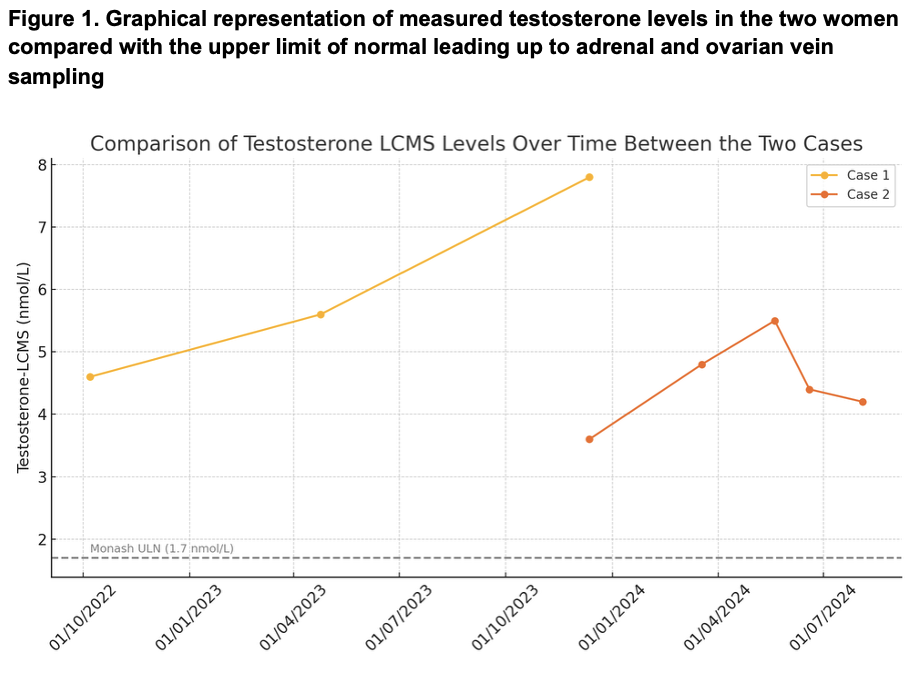
Case 1 was a 67-year-old woman with progressive androgenic alopecia and hirsutism (Ferriman-Gallwey score 30), with testosterone levels rising to 7.8 nmol/L (Table 1). Pelvic imaging was unremarkable, and an 11 mm indeterminate adrenal nodule was identified. OVS demonstrated a significant testosterone gradient in the left ovarian vein (Table 2). She was referred for bilateral oophorectomy, which is pending.
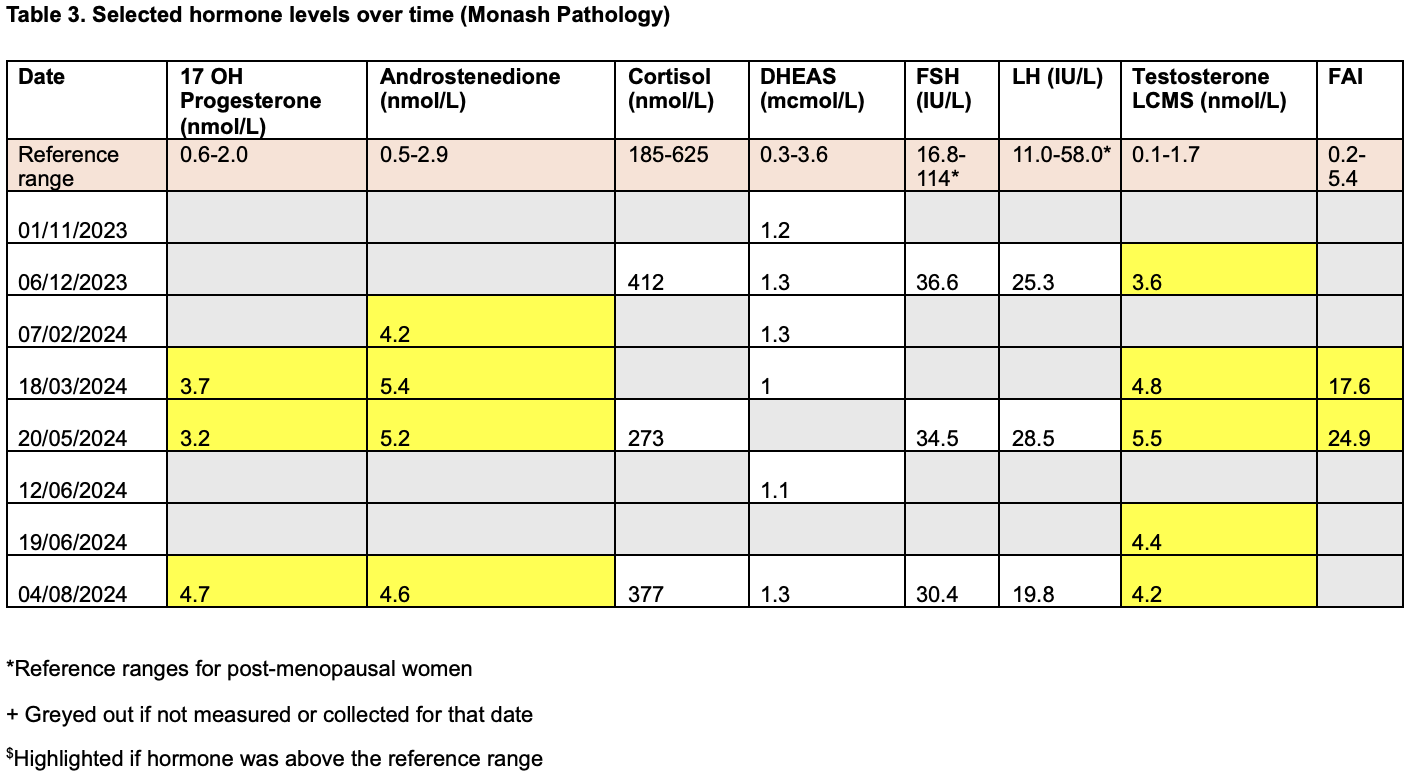
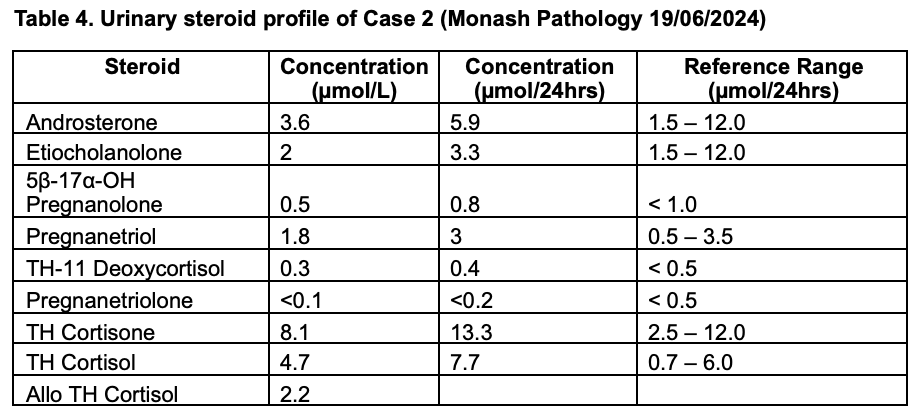
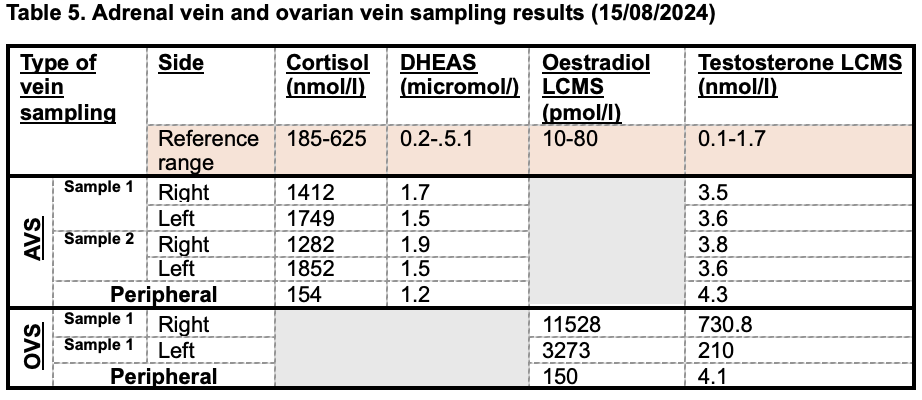
Case 2 was a 54-year-old woman with deepening of the voice and worsening hirsutism (Ferriman-Gallwey score 19), with persistently elevated serial serum testosterone, androstenedione, and free androgen index levels (Table 3). Imaging revealed a non-functioning adrenal adenoma but no ovarian abnormality. A urinary steroid profile (Table 4) was largely normal, with no evidence of congenital adrenal hyperplasia. Subsequent AVS/OVS results are outlined in Table 5, with biochemistry suggestive of a testosterone gradient consistent with an ovarian source. She was referred for bilateral oophorectomy, and histopathology confirmed bilateral ovarian stromal hyperthecosis.
Conclusion
Both cases demonstrate the utility of adrenal and ovarian vein sampling in the diagnostic algorithm of investigating imaging-negative causes of hyperandrogenism in post-menopausal women (1). Both patients had biochemical profiles concerning for androgen-secreting pathology despite inconclusive imaging. Testosterone levels significantly above the upper limit for postmenopausal women are highly suggestive of an androgen-secreting tumour or ovarian hyperthecosis (2).Selective venous sampling provided diagnostic clarity and influenced clinical decision-making.
- Elhassan YS, Hawley JM, Cussen L, et al. Society for Endocrinology Clinical Practice Guideline for the Evaluation of Androgen Excess in Women. Clin Endocrinol (Oxf). Published online 2025. doi:10.1111/cen.15265
- Shakir MKM, Snitchler AN, Vietor NO, Mai VQ, Hoang TD. Bilateral ovarian Leydig cell tumors in a postmenopausal woman causing hirsutism and virilization. AACE Clin Case Rep. 2021;7(1):26-28. doi:10.1016/j.aace.2020.11.004