Oral Presentation ESA-SRB-ANZOS 2025 in conjunction with ENSA
Increase in serum copeptin following treatment of hyponatraemia with tolvaptan: Secondary analysis of an open-label, randomised, clinical trial (128676)
Hyponatraemia is a common electrolyte disorder with significant morbidity, often driven by excess arginine vasopressin(AVP)(1). Copeptin is co-secreted with AVP but more stable and easily measured. Copeptin is not routinely measured in hyponatraemia as it is not useful in differentiating between common causes(2). It is not known whether hyponatremia treatment impacts copeptin concentration, or whether higher baseline copeptin may be associated with risk of overcorrection of plasma sodium(pNa) in patients treated with tolvaptan, an AVP-V2 receptor antagonist.
We conducted a three-day, randomised, single-centre, open-label trial comparing two hyponatraemia therapies, Tolvaptan and Fluid Restriction(FR), in hospitalised patients with pNa 115-130mmol/L. Copeptin measurement was performed on Day 1 and Day 4 on frozen serum using the BRAHMS Copeptin proAVP Kryptor assay from Thermo Fisher Scientific at Northern Health Pathology, Victoria.
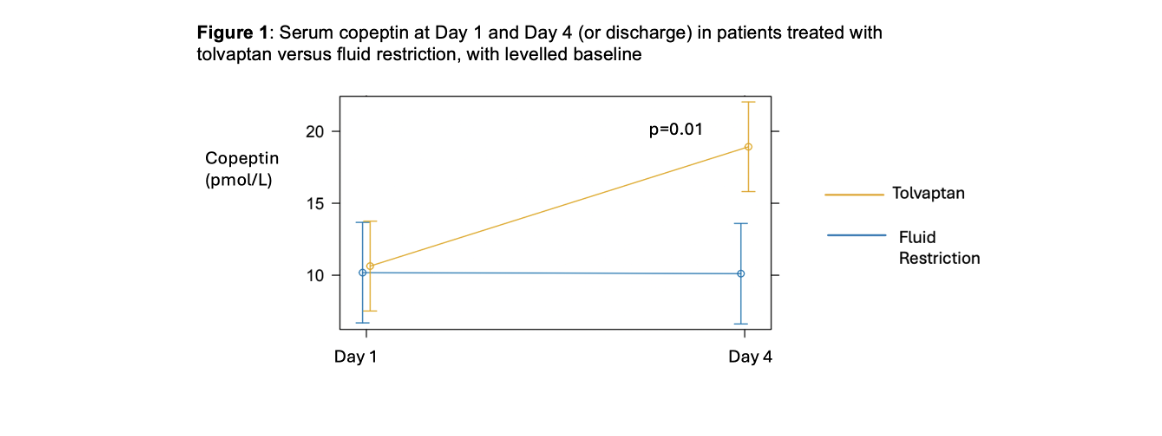
Fifty-four patients with mean pNa 123.8mmol/L were enrolled and randomised to tolvaptan (n=28) or FR (n=26). Serum copeptin was higher at baseline in participants randomised to tolvaptan (13.1 vs. 7.0pmol/L) by chance. Plasma sodium increased over 3 days in both arms, but significantly more with tolvaptan than FR (p.overall<0.001) as previously reported. Copeptin significantly increased in the tolvaptan group at Day 4, but remained stable with FR. The mean adjusted difference in copeptin between groups at Day 4 was 8.4pmol/L (95% CI 2.1-14.6,p=0.01)(Fig 1). There was no association between baseline copeptin concentration and rapid pNa rise, observed in 5 tolvaptan recipients.
Tolvaptan was associated with in an increase in serum copeptin that was not seen with fluid restriction, despite increased pNa in both groups. This suggests that AVP receptor blockade increased AVP production, but this did not compromise improvement in pNa. Contrary to expectation, higher baseline copeptin did not predict rapid pNa rise following tolvaptan. Further research is required to determine if there is clinical utility in measuring copeptin in hyponatraemia.
- Warren AM, Grossmann M, Christ-Crain M, Russell N. Syndrome of Inappropriate Antidiuresis: From Pathophysiology to Management. Endocr Rev. 2023.
- Fenske W, Störk S, Blechschmidt A, Maier SG, Morgenthaler NG, Allolio B. Copeptin in the differential diagnosis of hyponatremia. J Clin Endocrinol Metab. 2009;94(1):123-9.